
Search
- Page Path
- HOME > Search
Original Articles
- Thyroid
Big Data Articles (National Health Insurance Service Database) - Graves’ Disease and the Risk of End-Stage Renal Disease: A Korean Population-Based Study
- Yoon Young Cho, Bongseong Kim, Dong Wook Shin, Hye Ryoun Jang, Bo-Yeon Kim, Chan-Hee Jung, Jae Hyeon Kim, Sun Wook Kim, Jae Hoon Chung, Kyungdo Han, Tae Hyuk Kim
- Endocrinol Metab. 2022;37(2):281-289. Published online April 6, 2022
- DOI: https://doi.org/10.3803/EnM.2021.1333
- 3,908 View
- 134 Download
- 2 Web of Science
- 3 Crossref
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader  ePub
ePub - Background
Hyperthyroidism is associated with an increased glomerular filtration rate (GFR) in the hyperdynamic state, which is reversible after restoring euthyroidism. However, long-term follow-up of renal dysfunction in patients with hyperthyroidism has not been performed.
Methods
This was a retrospective cohort study using the Korean National Health Insurance database and biannual health checkup data. We included 41,778 Graves’ disease (GD) patients and 41,778 healthy controls, matched by age and sex. The incidences of end-stage renal disease (ESRD) were calculated in GD patients and controls. The cumulative dose and duration of antithyroid drugs (ATDs) were calculated for each patient and categorized into the highest, middle, and lowest tertiles.
Results
Among 41,778 GD patients, 55 ESRD cases occurred during 268,552 person-years of follow-up. Relative to the controls, regardless of smoking, drinking, or comorbidities, including chronic kidney disease, GD patients had a 47% lower risk of developing ESRD (hazard ratio [HR], 0.53; 95% confidence interval [CI], 0.37 to 0.76). In particular, GD patients with a higher baseline GFR (≥90 mL/min/1.73 m2; HR, 0.33; 95% CI, 0.11 to 0.99), longer treatment duration (>33 months; HR, 0.31; 95% CI, 0.17 to 0.58) or higher cumulative dose (>16,463 mg; HR, 0.29; 95% CI, 0.15 to 0.57) of ATDs had a significantly reduced risk of ESRD.
Conclusion
This was the first epidemiological study on the effect of GD on ESRD, and we demonstrated that GD population had a reduced risk for developing ESRD. -
Citations
Citations to this article as recorded by
- Renal function changes in patients with subclinical hyperthyroidism: a novel postulated mechanism
Magdy Mohamed Allam, Hanaa Tarek El-Zawawy, Tarek Hussein El-Zawawy
Endocrine.2023; 82(1): 78. CrossRef - Effect of Hyperthyroidism on Preventing Renal Insufficiency
Tae Yong Kim
Endocrinology and Metabolism.2022; 37(2): 220. CrossRef - Effects and Clinical Value of Peritoneal Dialysis on Water and Water Balance, Adverse Reactions, Quality of Life, and Clinical Prognosis in Patients with Decompensated Chronic Nephropathy: A Systematic Review and Meta-Analysis
Xichao Wang, Miaomiao Zhang, Na Sun, Wenxiu Chang, Gang Chen
Computational and Mathematical Methods in Medicine.2022; 2022: 1. CrossRef
- Renal function changes in patients with subclinical hyperthyroidism: a novel postulated mechanism

- Clinical Study
- Relationship of Sarcopenia with Microcirculation Measured by Skin Perfusion Pressure in Patients with Type 2 Diabetes
- Chan-Hee Jung, Yoon Young Cho, Dughyun Choi, Bo-Yeon Kim, Chul-Hee Kim, Ji-Oh Mok
- Endocrinol Metab. 2020;35(3):578-586. Published online September 22, 2020
- DOI: https://doi.org/10.3803/EnM.2020.679
- 5,384 View
- 122 Download
- 4 Web of Science
- 4 Crossref
-
Abstract
PDF
 Supplementary MaterialPubReader ePub
Supplementary MaterialPubReader ePub - Background
Few studies have examined the relationship of sarcopenia with the microcirculation. The current study investigated the relationship of sarcopenia with microcirculatory function, as assessed by skin perfusion pressure (SPP), in type 2 diabetes mellitus (T2DM) patients.
Methods
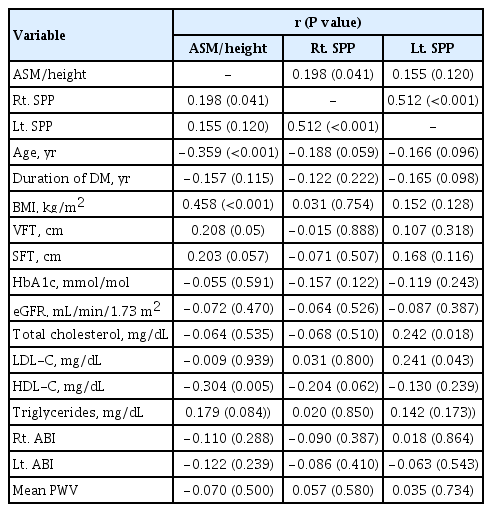
In total, 102 T2DM patients who underwent SPP measurements and bioelectrical impedance analysis (BIA) were enrolled in this cross-sectional study. SPP was assessed using the laser Doppler technique. Sarcopenia was defined as low height-adjusted appendicular muscle mass (men, <7 kg/m2; women, <5.7 kg/m2) using BIA. We divided the participants into two groups based on SPP (≤50 and >50 mm Hg), and an SPP below 50 mm Hg was considered to reflect impaired microcirculation.
Results
Fourteen patients (13.7%) were diagnosed with impaired microcirculatory function of the lower limb based on SPP. The prevalence of sarcopenia in all subjects was 11.8%, but the percentage of patients with an SPP ≤50 mm Hg who had sarcopenia was more than triple that of patients with an SPP >50 mm Hg (28.6% vs. 9.1%, P=0.036). A significant positive correlation was found between SPP and appendicular muscle mass adjusted for height (P=0.041 for right-sided SPP). Multiple logistic regression analysis showed that patients with sarcopenia had an odds ratio of 4.1 (95% confidence interval, 1.01 to 24.9) for having an SPP ≤50 mm Hg even after adjustment for confounding factors.
Conclusion
These results suggest that sarcopenia may be significantly associated with impaired microcirculation in patients with T2DM. Nonetheless, the small number of patients and wide CI require cautious interpretation of the results. -
Citations
Citations to this article as recorded by- Preclinical study of diabetic foot ulcers: From pathogenesis to vivo/vitro models and clinical therapeutic transformation
Yuqing Du, Jie Wang, Weijing Fan, Renyan Huang, Hongfei Wang, Guobin Liu
International Wound Journal.2023; 20(10): 4394. CrossRef - Bioelectrical Impedance Analysis for the Assessment of Body Composition in Sarcopenia and Type 2 Diabetes
Stefano Sbrignadello, Christian Göbl, Andrea Tura
Nutrients.2022; 14(9): 1864. CrossRef - Discrimination between possible sarcopenia and metabolic syndrome using the arterial pulse spectrum and machine-learning analysis
Li-Wei Wu, Te OuYoung, Yu-Chih Chiu, Ho-Feng Hsieh, Hsin Hsiu
Scientific Reports.2022;[Epub] CrossRef - The prevalence and risk factors of sarcopenia in patients with type 2 diabetes mellitus: a systematic review and meta-analysis
Yaqin Ai, Ruoxin Xu, Lingping Liu
Diabetology & Metabolic Syndrome.2021;[Epub] CrossRef
- Preclinical study of diabetic foot ulcers: From pathogenesis to vivo/vitro models and clinical therapeutic transformation
- Thyroid
- Prognosis of Differentiated Thyroid Carcinoma with Initial Distant Metastasis: A Multicenter Study in Korea
- Hosu Kim, Hye In Kim, Sun Wook Kim, Jaehoon Jung, Min Ji Jeon, Won Gu Kim, Tae Yong Kim, Hee Kyung Kim, Ho-Cheol Kang, Ji Min Han, Yoon Young Cho, Tae Hyuk Kim, Jae Hoon Chung
- Endocrinol Metab. 2018;33(2):287-295. Published online June 21, 2018
- DOI: https://doi.org/10.3803/EnM.2018.33.2.287
- 5,453 View
- 59 Download
- 31 Web of Science
- 28 Crossref
-
Abstract
PDFPubReader ePub
Background Most patients with differentiated thyroid cancer (DTC) have a favorable prognosis. However, patients with DTC and initial distant metastasis have not been commonly found, and their clinical characteristics have seldom been reported. In this study, we analyzed the clinical features and prognosis of patients with DTC and initial distant metastasis in Korea.
Methods We retrospectively reviewed the clinical data of 242 patients with DTC and initial distant metastasis treated from 1994 to 2013, collected from five tertiary hospitals in Korea.
Results The patients' median age was 51 years, and 65% were women. They were followed for a median of 7 years. Lung was the most common site of distant metastasis: only lung 149 patients (62%), only bone 49 (20%), other single site one (pleura), and combined sites 43 (40 were lung and bone, two were bone and other site, and one was lung and other site). At the time of diagnosis, 50 patients (21%) had non-radioactive iodine (RAI) avidity. Five-year disease-specific survival (DSS) was 85% and 10-year DSS was 68%, which were better than those in previous studies. After multivariate analysis, old age, male sex, metastatic site, and histologic type (follicular type) were significant factors for poor prognosis. However, negative RAI avidity status was not a significant prognostic factor after adjusting for other variables.
Conclusion The prognosis of Korean patients with DTC and initial distant metastasis was better than in previous studies. Old age, male sex, metastasis site, and histologic type were significant prognostic factors.
-
Citations
Citations to this article as recorded by- Case report: A case of hyperthyroidism secondary to bone metastasis of differentiated thyroid cancer
Tingyu Gu, Zhihong Zhao, Yuanyuan Shi, Zhenhua Sun, Yao Wang, Zhiyuan He, Kun Wang
Frontiers in Oncology.2024;[Epub] CrossRef - Theranostics of Thyroid Cancer
Luca Giovanella, Murat Tuncel, Atena Aghaee, Alfredo Campenni, Armando De Virgilio, Petra Petranović Ovčariček
Seminars in Nuclear Medicine.2024;[Epub] CrossRef - Thyroid Hormone Withdrawal versus Recombinant Human TSH as Preparation for I-131 Therapy in Patients with Metastatic Thyroid Cancer: A Systematic Review and Meta-Analysis
Luca Giovanella, Maria Luisa Garo, Alfredo Campenní, Petra Petranović Ovčariček, Rainer Görges
Cancers.2023; 15(9): 2510. CrossRef - Molecular Theranostics in Radioiodine-Refractory Differentiated Thyroid Cancer
Petra Petranović Ovčariček, Alfredo Campenni, Bart de Keizer, Desiree Deandreis, Michael C. Kreissl, Alexis Vrachimis, Murat Tuncel, Luca Giovanella
Cancers.2023; 15(17): 4290. CrossRef - Differentiating pulmonary metastasis from benign lung nodules in thyroid cancer patients using dual-energy CT parameters
Taeho Ha, Wooil Kim, Jaehyung Cha, Young Hen Lee, Hyung Suk Seo, So Young Park, Nan Hee Kim, Sung Ho Hwang, Hwan Seok Yong, Yu-Whan Oh, Eun-Young Kang, Cherry Kim
European Radiology.2022; 32(3): 1902. CrossRef - Feasibility of Recombinant Human TSH as a Preparation for Radioiodine Therapy in Patients with Distant Metastases from Papillary Thyroid Cancer: Comparison of Long-Term Survival Outcomes with Thyroid Hormone Withdrawal
Hsi-Chen Tsai, Kung-Chu Ho, Shih-Hsin Chen, Jing-Ren Tseng, Lan-Yan Yang, Kun-Ju Lin, Ju-Chin Cheng, Miaw-Jene Liou
Diagnostics.2022; 12(1): 221. CrossRef - Long-Term Quality of Life (5-15 Years Post-Thyroidectomy) of Thyroid Carcinoma Patients in Two Tertiary Care Hospitals
Mohammed Yousef Alyousef, Mohammed Khaled Ghandour, Mohammed Al-Mohawes, Mosaad Alnwaisir, Tahera Islam, Khalid Al Qahtani
Cureus.2022;[Epub] CrossRef - Evaluation of Lipocalin-2 and Twist expression in thyroid cancers and its relationship with epithelial mesenchymal transition
Pınar Celepli, İrem Bigat, Sefika Karabulut, Salih Celepli, Sema Hücümenoğlu
Annals of Diagnostic Pathology.2022; 59: 151973. CrossRef - Clinical study of ultrasonic evaluation of T/N staging of differentiated thyroid carcinoma using AJCC 8th staging criteria
Yu Liang, Xingxiang Huang, Zhe Song, Yang Yang, Ju Lei, Mei Ren, Li Tan, Hui Zhang, Francis Moore
PLOS ONE.2022; 17(6): e0269994. CrossRef - Therapeutic challenges in metastatic follicular thyroid cancer occurring in pregnancy: A case report
Claudio Spinelli, Beatrice Sanna, Marco Ghionzoli, Elisabetta Micelli
World Journal of Obstetrics and Gynecology.2022; 11(3): 33. CrossRef - Initial clinical and treatment patterns of advanced differentiated thyroid cancer: ERUDIT study
Juan Antonio Vallejo Casas, Marcel Sambo, Carlos López López, Manuel Durán-Poveda, Julio Rodríguez-Villanueva García, Rita Joana Santos, Marta Llanos, Elena Navarro-González, Javier Aller, Virginia Pubul, Sonsoles Guadalix, Guillermo Crespo, Cintia Gonzál
European Thyroid Journal.2022;[Epub] CrossRef - Male sex is not an independent risk factor for recurrence of differentiated thyroid cancer: a propensity score-matching study
Joonseon Park, Kwangsoon Kim, Dong-Jun Lim, Ja Seong Bae, Jeong Soo Kim
Scientific Reports.2021;[Epub] CrossRef - Evaluation of the 2015 ATA Guidelines in Patients With Distant Metastatic Differentiated Thyroid Cancer
Evert F S van Velsen, Merel T Stegenga, Folkert J van Kemenade, Boen L R Kam, Tessa M van Ginhoven, W Edward Visser, Robin P Peeters
The Journal of Clinical Endocrinology & Metabolism.2020; 105(3): e457. CrossRef - Usefulness of a 3D‐Printed Thyroid Cancer Phantom for Clinician to Patient Communication
Dayeong Hong, Sangwook Lee, Taehun Kim, Jung Hwan Baek, Won Woong Kim, Ki‐Wook Chung, Namkug Kim, Tae‐Yon Sung
World Journal of Surgery.2020; 44(3): 788. CrossRef - Estimating the Growth Rate of Lung Metastases in Differentiated Thyroid Carcinoma: Response Evaluation Criteria in Solid Tumors or Doubling Time?
Eyun Song, Jonghwa Ahn, Min Ji Jeon, Sang Min Lee, Jeong Hyun Lee, Tae Yong Kim, Jung Hwan Baek, Won Bae Kim, Young Kee Shong, Won Gu Kim
Thyroid.2020; 30(3): 418. CrossRef - Personalized management of differentiated thyroid cancer in real life – practical guidance from a multidisciplinary panel of experts
Alfredo Campennì, Daniele Barbaro, Marco Guzzo, Francesca Capoccetti, Luca Giovanella
Endocrine.2020; 70(2): 280. CrossRef - Unusual metastases from differentiated thyroid cancers: A multicenter study in Korea
Jee Hee Yoon, Min Ji Jeon, Mijin Kim, A. Ram Hong, Hee Kyung Kim, Dong Yeob Shin, Bo Hyun Kim, Won Bae Kim, Young Kee Shong, Ho-Cheol Kang, Domenico Albano
PLOS ONE.2020; 15(8): e0238207. CrossRef - Extended Real-World Observation of Patients Treated with Sorafenib for Radioactive Iodine-Refractory Differentiated Thyroid Carcinoma and Impact of Lenvatinib Salvage Treatment: A Korean Multicenter Study
Hye-Seon Oh, Dong Yeob Shin, Mijin Kim, So Young Park, Tae Hyuk Kim, Bo Hyun Kim, Eui Young Kim, Won Bae Kim, Jae Hoon Chung, Young Kee Shong, Dong Jun Lim, Won Gu Kim
Thyroid.2019; 29(12): 1804. CrossRef - Clinical outcomes and prognostic factors in patients with no less than three distant organ system metastases from differentiated thyroid carcinoma
Xin-Yun Zhang, Jian-Wen Sun, Zhong-Ling Qiu, Yang Wang, Xiao-Yue Chen, Jin-Hua Zhao, Quan-Yong Luo
Endocrine.2019; 66(2): 254. CrossRef - Molecular Profile and Clinical Outcomes in Differentiated Thyroid Cancer Patients Presenting with Bone Metastasis
Nilma Malik, Alyaksandr V. Nikitski, Elie Klam, Jason Hunt, Benjamin Witt, Barbara Chadwick, Yuri E. Nikiforov, Devaprabu Abraham
Endocrine Practice.2019; 25(12): 1255. CrossRef - Improved survival after early detection of asymptomatic distant metastasis in patients with thyroid cancer
Hosu Kim, So Young Park, Jaehoon Jung, Jung-Han Kim, Soo Yeon Hahn, Jung Hee Shin, Young Lyun Oh, Man Ki Chung, Hye In Kim, Sun Wook Kim, Jae Hoon Chung, Tae Hyuk Kim
Scientific Reports.2019;[Epub] CrossRef - Unusual metastases from differentiated thyroid carcinoma: analysis of 36 cases
Anabela Zunino, Fabián Pitoia, Eduardo Faure, Adriana Reyes, Mónica Sala, Rosana Sklate, Verónica Ilera, Inés Califano
Endocrine.2019; 65(3): 630. CrossRef - The Prognosis of Papillary Thyroid Cancer with Initial Distant Metastasis is Strongly Associated with Extensive Extrathyroidal Extension: A Retrospective Cohort Study
Young Ki Lee, Daham Kim, Dong Yeob Shin, Cho Rok Lee, Eun Jig Lee, Sang-Wook Kang, Jandee Lee, Jong Ju Jeong, Kee-Hyun Nam, Woong Youn Chung, Cheong Soo Park
Annals of Surgical Oncology.2019; 26(7): 2200. CrossRef - Risk Factors for Distant Metastasis in Follicular Thyroid Carcinoma in Korea
Shin Dol Jo, Joon-Hyop Lee, Suk Ha Kang, Yun Yeong Kim, Yong Soon Chun, Heung Kyu Park, Sang Tae Choi, Jin Mo Kang, Yoo Seung Chung
Journal of Endocrine Surgery.2019; 19(1): 1. CrossRef - Expression levels of ARHI and Beclin1 in thyroid cancer and their relationship with clinical pathology and prognosis
Houwei Zhu, Yanqing Qu
Oncology Letters.2019;[Epub] CrossRef - 甲状腺腫瘍治療の最新情報
Nippon Jibiinkoka Gakkai Kaiho.2018; 121(11): 1336. CrossRef - Clinical Outcomes of Differentiated Thyroid Cancer Patients with Local Recurrence or Distant Metastasis Detected in Old Age
Ji Min Han, Ji Cheol Bae, Hye In Kim, Sam Kwon, Min Ji Jeon, Won Gu Kim, Tae Yong Kim, Young Kee Shong, Won Bae Kim
Endocrinology and Metabolism.2018; 33(4): 459. CrossRef - Efficacy and Affecting Factors of 131I Thyroid Remnant Ablation After Surgical Treatment of Differentiated Thyroid Carcinoma
Chen Wang, Hongcui Diao, Ping Ren, Xufu Wang, Yangang Wang, Wenjuan Zhao
Frontiers in Oncology.2018;[Epub] CrossRef
- Case report: A case of hyperthyroidism secondary to bone metastasis of differentiated thyroid cancer
- Clinical Study
- Economic Evaluation of Recombinant Human Thyroid Stimulating Hormone Stimulation vs. Thyroid Hormone Withdrawal Prior to Radioiodine Ablation for Thyroid Cancer: The Korean Perspective
- Seo Young Sohn, Hye Won Jang, Yoon Young Cho, Sun Wook Kim, Jae Hoon Chung
- Endocrinol Metab. 2015;30(4):531-542. Published online December 31, 2015
- DOI: https://doi.org/10.3803/EnM.2015.30.4.531
- 3,544 View
- 43 Download
- 9 Web of Science
- 8 Crossref
-
Abstract
PDFPubReader
Background Previous studies have suggested that recombinant human thyroid stimulating hormone (rhTSH) stimulation is an acceptable alternative to thyroid hormone withdrawal (THW) when radioiodine remnant ablation is planned for thyroid cancer treatment, based on superior short-term quality of life with non-inferior remnant ablation efficacy. This study evaluated the cost-effectiveness of radioiodine remnant ablation using rhTSH, compared with the traditional preparation method which renders patients hypothyroid by THW, in Korean perspective.
Methods This economic evaluation considered the costs and benefits to the Korean public healthcare system. Clinical experts were surveyed regarding the current practice of radioiodine ablation in Korea and their responses helped inform assumptions used in a cost effectiveness model. Markov modelling with 17 weekly cycles was used to assess the incremental costs per quality-adjusted life year (QALY) associated with rhTSH. Clinical inputs were based on a multi-center, randomized controlled trial comparing remnant ablation success after rhTSH preparation with THW. The additional costs associated with rhTSH were considered relative to the clinical benefits and cost offsets.
Results The additional benefits of rhTSH (0.036 QALY) are achieved with an additional cost of Korean won ₩961,105, equating to cost per QALY of ₩26,697,361. Sensitivity analyses had only a modest impact upon cost-effectiveness, with one-way sensitivity results of approximately ₩33,000,000/QALY.
Conclusion The use of rhTSH is a cost-effective alternative to endogenous hypothyroid stimulation prior to radioiodine ablation for patients who have undergone thyroidectomy in Korea.
-
Citations
Citations to this article as recorded by- Comparison of Recombinant Human Thyroid-Stimulating Hormone and Thyroid Hormone Withdrawal for 131I Therapy in Patients With Intermediate- to High-Risk Thyroid Cancer
Sohyun Park, Ji-In Bang, Keunyoung Kim, Youngduk Seo, Ari Chong, Chae Moon Hong, Dong-Eun Lee, Miyoung Choi, Sang-Woo Lee, So Won Oh
Clinical Nuclear Medicine.2024; 49(3): e96. CrossRef - Thyroid Hormone Withdrawal versus Recombinant Human TSH as Preparation for I-131 Therapy in Patients with Metastatic Thyroid Cancer: A Systematic Review and Meta-Analysis
Luca Giovanella, Maria Luisa Garo, Alfredo Campenní, Petra Petranović Ovčariček, Rainer Görges
Cancers.2023; 15(9): 2510. CrossRef - Health-related quality of life of thyroid cancer patients undergoing radioiodine therapy: a cohort real-world study in a reference public cancer hospital in Brazil
Jayda Eiras Ramim, Marcella Araugio Soares Cardoso, Gessen Lopes Carneiro de Oliveira, Maria Luisa Gomes, Tiago Teixeira Guimarães, Rossana Corbo Ramalho de Mello, Anke Bergmann, Priscilla Brunelli Pujatti
Supportive Care in Cancer.2020; 28(8): 3771. CrossRef - Predictive factors determining incomplete response to radioiodine therapy in patients with differentiated thyroid cancer
Ewelina Szczepanek-Parulska, Magdalena Wojewoda-Korbelak, Martyna Borowczyk, Malgorzata Kaluzna, Barbara Brominska, Katarzyna Ziemnicka, Rafal Czepczynski, Maciej Baczyk, Marek Ruchala
The Quarterly Journal of Nuclear Medicine and Molecular Imaging.2020;[Epub] CrossRef - Initial Adoption of Recombinant Human Thyroid-Stimulating Hormone Following Thyroidectomy in the Medicare Thyroid Cancer Patient Population
Michaela A. Dinan, Yanhong Li, Shelby D. Reed, Julie Ann Sosa
Endocrine Practice.2019; 25(1): 31. CrossRef - Triennial Report ofEndocrinology and Metabolism, 2015 to 2017
Eun-Jung Rhee, Hey Yeon Jang, Won-Young Lee
Endocrinology and Metabolism.2018; 33(2): 195. CrossRef - Recombinant human TSH stimulated thyroglobulin levels at remnant ablation predict structural incomplete response to treatment in patients with differentiated thyroid cancer
Jeonghoon Ha, Min Hee Kim, Kwanhoon Jo, Yejee Lim, Ja Seong Bae, Sohee Lee, Moo Il Kang, Bong Yun Cha, Dong Jun Lim
Medicine.2017; 96(29): e7512. CrossRef - Does the Risk of Metabolic Syndrome Increase in Thyroid Cancer Survivors?
Min-Hee Kim, Jin-young Huh, Dong-jun Lim, Moo-Il Kang
Thyroid.2017; 27(7): 936. CrossRef
- Comparison of Recombinant Human Thyroid-Stimulating Hormone and Thyroid Hormone Withdrawal for 131I Therapy in Patients With Intermediate- to High-Risk Thyroid Cancer
- Thyroid
- Weight Changes in Patients with Differentiated Thyroid Carcinoma during Postoperative Long-Term Follow-up under Thyroid Stimulating Hormone Suppression
- Seo Young Sohn, Ji Young Joung, Yoon Young Cho, Sun Mi Park, Sang Man Jin, Jae Hoon Chung, Sun Wook Kim
- Endocrinol Metab. 2015;30(3):343-351. Published online August 4, 2015
- DOI: https://doi.org/10.3803/EnM.2015.30.3.343
- 4,093 View
- 60 Download
- 10 Web of Science
- 14 Crossref
-
Abstract
PDFPubReader
Background There are limited data about whether patients who receive initial treatment for differentiated thyroid cancer (DTC) gain or lose weight during long-term follow-up under thyroid stimulating hormone (TSH) suppression. This study was aimed to evaluate whether DTC patients under TSH suppression experience long-term weight gain after initial treatment. We also examined the impact of the radioactive iodine ablation therapy (RAIT) preparation method on changes of weight, comparing thyroid hormone withdrawal (THW) and recombinant human TSH (rhTSH).
Methods We retrospectively reviewed 700 DTC patients who underwent a total thyroidectomy followed by either RAIT and levothyroxine (T4) replacement or T4 replacement alone. The control group included 350 age-matched patients with benign thyroid nodules followed during same period. Anthropometric data were measured at baseline, 1 to 2 years, and 3 to 4 years after thyroidectomy. Comparisons were made between weight and body mass index (BMI) at baseline and follow-up.
Results Significant gains in weight and BMI were observed 3 to 4 years after initial treatment for female DTC but not in male patients. These gains among female DTC patients were also significant compared to age-matched control. Women in the THW group gained a significant amount of weight and BMI compared to baseline, while there was no increase in weight or BMI in the rhTSH group. There were no changes in weight and BMI in men according to RAIT preparation methods.
Conclusion Female DTC patients showed significant gains in weight and BMI during long-term follow-up after initial treatment. These changes were seen only in patients who underwent THW for RAIT.
-
Citations
Citations to this article as recorded by- Impact of a mobile health intervention based on multi-theory model of health behavior change on self-management in patients with differentiated thyroid cancer: protocol for a randomized controlled trial
Yang Jiang, Xiangju Sun, Maomin Jiang, Hewei Min, Jing Wang, Xinghua Fu, Jiale Qi, Zhenjie Yu, Xiaomei Zhu, Yibo Wu
Frontiers in Public Health.2024;[Epub] CrossRef - Thyroidectomy Effects on the Body Mass Index and Thyroid-Stimulating Hormone: A Systematic Review and Meta-Analysis
Hyder Mirghani, Ahmad M Fnjan, Abdullah F Almalki, Ali F Almadan, Omar Abdullah M Alammar, Abdulaziz S Alhwiati, Amer A Laradhi, Ahmed M Bakour, Mohamad A Aljahed, Abdulmajeed M Alzahrani
Cureus.2024;[Epub] CrossRef - Pre-surgery dietician counseling can prevent post-thyroidectomy body weight gain: results of an intervention trial
Laura Croce, Cristina Pallavicini, Noemi Busca, Benedetto Calì, Giuseppe Bellastella, Francesca Coperchini, Flavia Magri, Luca Chiovato, Hellas Cena, Mario Rotondi
Endocrine.2023; 81(2): 246. CrossRef - Determinants and mediating mechanisms of quality of life and disease-specific symptoms among thyroid cancer patients: the design of the WaTCh study
Floortje Mols, Dounya Schoormans, Romana Netea-Maier, Olga Husson, Sandra Beijer, Katrijn Van Deun, Wouter Zandee, Marleen Kars, Pleun C. M. Wouters van Poppel, Suat Simsek, Patrick van Battum, Jérôme M. H. Kisters, Jan Paul de Boer, Elske Massolt, Rachel
Thyroid Research.2023;[Epub] CrossRef - Effects of a low-iodine diet in post-thyroidectomy thyroid cancer patients undergoing I131 therapy at the Vietnam National Cancer Hospital
Bach Viet Hoang, Tien Thi Hong Nguyen, Yen Thi Duong, Hoa Thi Thanh Nguyen, Thu Ha Nguyen, Thanh Thi Nguyen, Lieu Thi Thu Nguyen, Huong Thi Le
Nutrition and Health.2023;[Epub] CrossRef - Positive effects of thyroid replacement therapy on assisted reproductive technology outcomes in women with subclinical hypothyroidism with positive thyroid peroxidase autoantibodies
Himanshu Arora, Ineabelle Collazo, Katherine L. Palmerola, Madhumita Parmar, Manish Narasimman, Nicholas Hendon, Juergen Eisermann, Maria Bustillo
F&S Reports.2022; 3(1): 32. CrossRef - Weight Gain After Thyroidectomy: A Systematic Review and Meta-Analysis
Christine N Huynh, Janina V Pearce, Le Kang, Francesco S Celi
The Journal of Clinical Endocrinology & Metabolism.2021; 106(1): 282. CrossRef - Weight change in patients with differentiated thyroid carcinoma after total thyroidectomy versus lobectomy
Hae-Ryong Cho, Ra-Yeong Song, Kyung Ho Kang
Korean Journal of Clinical Oncology.2020; 16(2): 127. CrossRef - Postthyroidectomy obesity in a Korean population: does the extent of surgery matter?
Min-Young Park, Sang Eun Nam, Kyoung Sik Park, Madhuri Saindane, Young-Bum Yoo, Jung-Hyun Yang, Ah-Leum Ahn, Jae-Kyung Choi, Won Seo Park
Annals of Surgical Treatment and Research.2019; 97(3): 119. CrossRef - Body weight change is unpredictable after total thyroidectomy
Ron Glick, Paula Chang, Peter Michail, Jonathan W. Serpell, Simon Grodski, James C. Lee
ANZ Journal of Surgery.2018; 88(3): 162. CrossRef - Weight Changes After Thyroid Surgery for Patients with Benign Thyroid Nodules and Thyroid Cancer: Population-Based Study and Systematic Review and Meta-Analysis
Naykky Singh Ospina, Ana Castaneda-Guarderas, Oksana Hamidi, Oscar J. Ponce, Wang Zhen, Larry Prokop, Victor M. Montori, Juan P. Brito
Thyroid.2018; 28(5): 639. CrossRef - Does the Risk of Metabolic Syndrome Increase in Thyroid Cancer Survivors?
Min-Hee Kim, Jin-young Huh, Dong-jun Lim, Moo-Il Kang
Thyroid.2017; 27(7): 936. CrossRef - Thyroid hormone and its metabolites in relation to quality of life in patients treated for differentiated thyroid cancer
E.T. Massolt, M. van der Windt, T.I.M. Korevaar, B.L.R. Kam, J.W. Burger, G.J.H. Franssen, I. Lehmphul, J. Köhrle, W.E. Visser, R.P. Peeters
Clinical Endocrinology.2016; 85(5): 781. CrossRef - High Serum Levels of Thyroid-Stimulating Hormone and Sustained Weight Gain in Patients with Thyroid Cancer Undergoing Radioiodine Therapy
Hyo Jung Seo, June-Key Chung, Keon Wook Kang, E. Edmund Kim, Gi Jeong Cheon, Jin Chul Paeng, Dong Soo Lee, Young Joo Park, Do Joon Park, Jae Gol Choe
International Journal of Thyroidology.2016; 9(1): 19. CrossRef
- Impact of a mobile health intervention based on multi-theory model of health behavior change on self-management in patients with differentiated thyroid cancer: protocol for a randomized controlled trial
- Adrenal gland
- Clinical Characteristics, Management, and Outcome of 22 Cases of Primary Hypophysitis
- Sun Mi Park, Ji Cheol Bae, Ji Young Joung, Yoon Young Cho, Tae Hun Kim, Sang-Man Jin, Sunghwan Suh, Kyu Yeon Hur, Kwang-Won Kim
- Endocrinol Metab. 2014;29(4):470-478. Published online December 29, 2014
- DOI: https://doi.org/10.3803/EnM.2014.29.4.470
- 4,250 View
- 41 Download
- 26 Web of Science
- 24 Crossref
-
Abstract
PDFPubReader
Background Primary hypophysitis causes varying degrees of endocrine dysfunction and mass effect. The natural course and best treatment have not been well established.
Methods Medical records of 22 patients who had been diagnosed with primary hypophysitis between January 2001 and March 2013 were retrospectively reviewed. Based on the anatomical location, we classified the cases as adenohypophysitis (AH), infundibuloneurohypophysitis (INH), and panhypophysitis (PH). Clinical presentation, endocrine function, pathologic findings, magnetic resonance imaging findings, and treatment courses were reviewed.
Results Among 22 patients with primary hypophysitis, 81.8% (18/22) had involvement of the posterior pituitary lobe. Two patients of the AH (2/3, 66.6%) and three patients of the PH (3/10, 30%) groups initially underwent surgical mass reduction. Five patients, including three of the PH (3/10, 33.3%) group and one from each of the AH (1/3, 33.3%) and INH (1/9, 11.1%) groups, initially received high-dose glucocorticoid treatment. Nearly all of the patients treated with surgery or high-dose steroid treatment (9/11, 82%) required continuous hormone replacement during the follow-up period. Twelve patients received no treatment for mass reduction due to the absence of acute symptoms and signs related to a compressive mass effect. Most of them (11/12, 92%) did not show disease progression, and three patients recovered partially from hormone deficiency.
Conclusion Deficits of the posterior pituitary were the most common features in our cases of primary hypophysitis. Pituitary endocrine defects responded less favorably to glucocorticoid treatment and surgery. In the absence of symptoms related to mass effect and with the mild defect of endocrine function, it may not require treatment to reduce mass except hormone replacement.
-
Citations
Citations to this article as recorded by- Secondary xanthogranulomatous hypophysitis mimicking a pituitary macroadenoma: a case report
Salma Salhi, Ibtissem Oueslati, Yasmine Mouelhi, Alia Zehani, Nidhameddine Kchir, Elyes Kamoun, Meriem Yazidi, Melika Chihaoui
Journal of International Medical Research.2024;[Epub] CrossRef - Glucocorticoid therapy as first-line treatment in primary hypophysitis: a systematic review and individual patient data meta-analysis
Brijesh Krishnappa, Ravikumar Shah, Saba Samad Memon, Chakra Diwaker, Anurag R Lila, Virendra A Patil, Nalini S Shah, Tushar R Bandgar
Endocrine Connections.2023;[Epub] CrossRef - Hypophysitis, the Growing Spectrum of a Rare Pituitary Disease
Fabienne Langlois, Elena V Varlamov, Maria Fleseriu
The Journal of Clinical Endocrinology & Metabolism.2022; 107(1): 10. CrossRef - Outcomes of Initial Management Strategies in Patients With Autoimmune Lymphocytic Hypophysitis: A Systematic Review and Meta-analysis
Diane Donegan, Zeb Saeed, Danae A Delivanis, Mohammad Hassan Murad, Juergen Honegger, Felix Amereller, Seda Hanife Oguz, Dana Erickson, Irina Bancos
The Journal of Clinical Endocrinology & Metabolism.2022; 107(4): 1170. CrossRef - Early Pulse Glucocorticoid Therapy and Improved Hormonal Outcomes in Primary Hypophysitis
Brijesh Krishnappa, Ravikumar Shah, Vijaya Sarathi, Anurag Ranjan Lila, Manjeet Kaur Sehemby, Virendra A. Patil, Shilpa Sankhe, Nalini Shah, Tushar Bandgar
Neuroendocrinology.2022; 112(2): 186. CrossRef - Preoperative differentiation of hypophysitis and pituitary adenomas using a novel clinicoradiologic scoring system
Kyla Wright, Hyon Kim, Travis Hill, Matthew Lee, Cordelia Orillac, Nikita Mogar, Donato Pacione, Nidhi Agrawal
Pituitary.2022; 25(4): 602. CrossRef - Hypophysitis
Diane Donegan, Jürgen Honegger
Endocrine Practice.2022; 28(9): 901. CrossRef - Rare Case of a Disappearing Pituitary Adenoma During the Coronavirus Disease 2019 (COVID-19) Pandemic
David P. Bray, C. Arturo Solares, Nelson M. Oyesiku
World Neurosurgery.2021; 146: 148. CrossRef - Diabetes insipidus secondary to sellar/parasellar lesions
Anna Angelousi, Chrysoula Mytareli, Paraskevi Xekouki, Eva Kassi, Konstantinos Barkas, Ashley Grossman, Gregory Kaltsas
Journal of Neuroendocrinology.2021;[Epub] CrossRef - Clinical presentation and management of hypophysitis: An observational study of case series
Marouan Karrou, Salma Benyakhlef, Achwak Alla, Najoua Messaoudi, Asmae Oulad Amar, Siham Rouf, Imane Kamaoui, Noureddine Oulali, Faycal Moufid, Naima Abda, Hanane Latrech
Surgical Neurology International.2021; 12: 304. CrossRef - Clinical aspects of autoimmune hypothalamitis, a variant of autoimmune hypophysitis: Experience from one center
Qian Wei, Guoqing Yang, Zhaohui Lue, Jingtao Dou, Li Zang, Yijun Li, Jin Du, Weijun Gu, Yiming Mu
Journal of International Medical Research.2020; 48(3): 030006051988783. CrossRef - Primary and Ipilimumab-induced Hypophysitis: A Single-center Case Series
Paul Atkins, Ehud Ur
Endocrine Research.2020; 45(4): 246. CrossRef - Hypophysitis (Including IgG4 and Immunotherapy)
Anna Angelousi, Krystallenia Alexandraki, Marina Tsoli, Gregory Kaltsas, Eva Kassi
Neuroendocrinology.2020; 110(9-10): 822. CrossRef - Hypophysitis in the era of immune checkpoint inhibitors and immunoglobulin G4-related disease
Leen Wehbeh, Sama Alreddawi, Roberto Salvatori
Expert Review of Endocrinology & Metabolism.2019; 14(3): 167. CrossRef - Immune check point inhibitors-induced hypophysitis: a retrospective analysis of the French Pharmacovigilance database
Julie Garon-Czmil, Nadine Petitpain, Franck Rouby, Marion Sassier, Samy Babai, Mélissa Yéléhé-Okouma, Georges Weryha, Marc Klein, Pierre Gillet
Scientific Reports.2019;[Epub] CrossRef - Clinical Features, Magnetic Resonance Imaging, and Treatment Experience of 20 Patients with Lymphocytic Hypophysitis in a Single Center
Qiang Zhu, Ke Qian, Guijun Jia, Gang Lv, Jisheng Wang, Liyong Zhong, Shuqing Yu
World Neurosurgery.2019; 127: e22. CrossRef - Idiopathic granulomatous hypophysitis presenting with galactorrhea, headache, and nausea in a woman: a case report and review of the literature
Guive Sharifi, Mohammad Reza Mohajeri-Tehrani, Behrouz Navabakhsh, Bagher Larijani, Touraj Valeh
Journal of Medical Case Reports.2019;[Epub] CrossRef - Paciente de 31 años con polidipsia
A.R. Benavides Aramburu, M. Seguí Díaz
Medicina de Familia. SEMERGEN.2018; 44(2): e77. CrossRef - Primary hypophysitis and other autoimmune disorders of the sellar and suprasellar regions
Sriram Gubbi, Fady Hannah-Shmouni, Constantine A. Stratakis, Christian A. Koch
Reviews in Endocrine and Metabolic Disorders.2018; 19(4): 335. CrossRef - Primary lymphocytic hypophysitis: Clinical characteristics and treatment of 50 cases in a single centre in China over 18 years
Shuchang Wang, Linjie Wang, Yong Yao, Feng Feng, Hongbo Yang, Zhiyong Liang, Kan Deng, Hui You, Jian Sun, Bing Xing, Zimeng Jin, Renzhi Wang, Hui Pan, Huijuan Zhu
Clinical Endocrinology.2017; 87(2): 177. CrossRef - Clinical presentation and outcome of children with central diabetes insipidus associated with a self‐limited or transient pituitary stalk thickening, diagnosed as infundibuloneurohypophysitis
J. Schaefers, M. Cools, K. De Waele, I. Gies, V. Beauloye, P. Lysy, I. Francois, D. Beckers, J. De Schepper
Clinical Endocrinology.2017; 87(2): 171. CrossRef - Intrachiasmatic abscess caused by IgG4-related hypophysitis
Georgios F. Hadjigeorgiou, Eva Løbner Lund, Lars Poulsgaard, Ulla Feldt-Rasmussen, Åse Krogh Rasmussen, Marianne Wegener, Kåre Fugleholm
Acta Neurochirurgica.2017; 159(11): 2229. CrossRef - Granulomatous and lymphocytic hypophysitis – are they immunologically distinct?
Shilpa Rao, Anita Mahadevan, Tanmoy Maiti, Manish Ranjan, Shivayogi Durgad Shwetha, Arimappamagan Arivazhagan, Jitender Saini
APMIS.2016; 124(12): 1072. CrossRef - Articles in 'Endocrinology and Metabolism' in 2014
Won-Young Lee
Endocrinology and Metabolism.2015; 30(1): 47. CrossRef
- Secondary xanthogranulomatous hypophysitis mimicking a pituitary macroadenoma: a case report
Case Reports
- Thyroid
- Steroid Responsive Xanthomatous Hypophysitis Associated with Autoimmune Thyroiditis: A Case Report
- Ji Young Joung, Hyemin Jeong, Yoon Young Cho, Kyoungmin Huh, Yeon-Lim Suh, Kwang-Won Kim, Ji Cheol Bae
- Endocrinol Metab. 2013;28(1):65-69. Published online March 25, 2013
- DOI: https://doi.org/10.3803/EnM.2013.28.1.65
- 3,484 View
- 30 Download
- 16 Crossref
-
Abstract
PDFPubReader
We report the case of a 36-year-old woman who presented with headache, fever, and amenorrhea. Laboratory analysis revealed hypopituitarism and autoimmune thyroiditis, while a cerebrospinal fluid study suggested concurrent aseptic meningitis. A magnetic resonance image (MRI) scan revealed a 1.0×0.9 cm cystic mass enlarging the sella turcica. Surgical resection via an endoscopic transsphenoidal route was performed. The histological finding of the excised tissue revealed foamy histiocytes with vacuolated cytoplasm, supporting the diagnosis of xanthomatous hypophysitis. Although a residual soft lesion was observed on the MRI image postoperatively, the patient's headache and fever improved. Ten months after surgery, the patient complained of visual impairment and headache, and the residual mass had enlarged into the suprasellar area. High dose (500 mg intravenous) methylprednisolone was administered for 3 days. During the methylprednisolone pulse therapy, the patient's visual acuity and headache improved. A follow-up MRI taken after methylprednisolone therapy showed a marked mass reduction. Our case supports an autoimmune pathophysiology for xanthomatous hypophysitis and suggests that high dose glucocorticoid therapy as a treatment option.
-
Citations
Citations to this article as recorded by- Xanthomatous hypophysitis causing hypogonadotropic hypogonadism resulting in delayed presentation of slipped capital femoral epiphysis
Kirit Singh, Avinash Kumar Kanodia, Peter Ross, Antonia Torgersen, Jamie Maclean, Graham Leese, Kismet Hossain-Ibrahim
British Journal of Neurosurgery.2022; 36(2): 286. CrossRef - Full recovery from chronic headache and hypopituitarism caused by lymphocytic hypophysitis: A case report
Mao-Guang Yang, Han-Qing Cai, Si-Si Wang, Lin Liu, Chun-Mei Wang
World Journal of Clinical Cases.2022; 10(3): 1041. CrossRef - Xanthomatous Hypophysitis Secondary to a Ruptured Rathke’s Cleft Cyst: A Case Report
Emre Gezer, Burak Çabuk, Büşra Yaprak Bayrak, Zeynep Cantürk, Berrin Çetinarslan, Alev Selek, Mehmet Sözen, Damla Köksalan, Savaş Ceylan
Brain Tumor Research and Treatment.2022; 10(1): 48. CrossRef - Successful immunomodulatory treatment for recurrent xanthogranulomatous hypophysitis in an adolescent: illustrative case
Sarah DeCou, Pablo F. Recinos, Richard A. Prayson, Christopher Karakasis, Anzar Haider, Neha Patel
Journal of Neurosurgery: Case Lessons.2022;[Epub] CrossRef - Xanthogranulomatous hypophysitis: A rare presentation in a young female patient
Mohammad Ali Yaghoubi, Samira Zabihyan, Amin Saeidinia, Masoumeh Gharib, Ramin Ghiyasi Moghaddam
Clinical Case Reports.2022;[Epub] CrossRef - Xanthomatous Hypophysitis Presenting in an Adolescent Girl: A Long-Term Follow-Up of a Rare Case and Review of the Literature
Jeanne Sze Lyn Wong, Azraai Bahari Nasruddin, Nalini M. Selveindran, Kartikasalwah Abd Latif, Fauziah Kassim, Sukanya Banerjee Nair, Janet Y.H. Hong
AACE Clinical Case Reports.2021; 7(3): 220. CrossRef - Xanthomatous Hypophysitis: A Case Report and Comprehensive Literature Review
Jianyu Zhu, Zhicheng Wang, Wenze Wang, Jinghua Fan, Yi Zhang, Xiaoxu Li, Jie Liu, Shenzhong Jiang, Kan Deng, Lian Duan, Yong Yao, Huijuan Zhu
Frontiers in Endocrinology.2021;[Epub] CrossRef - Recurring Primary Xanthomatous Hypophysitis Behaving Like Pituitary Adenoma: Additional Case and Literature Review
Mansour Mathkour, Tyler Zeoli, Cassidy Werner, Tyler Scullen, Juanita Garces, Joseph Keen, Marcus Ware
World Neurosurgery.2020; 138: 27. CrossRef - Imaging findings in hypophysitis: a review
Ferdinando Caranci, Giuseppe Leone, Andrea Ponsiglione, Massimo Muto, Fabio Tortora, Mario Muto, Sossio Cirillo, Luca Brunese, Alfonso Cerase
La radiologia medica.2020; 125(3): 319. CrossRef - Hypophysitis in the era of immune checkpoint inhibitors and immunoglobulin G4-related disease
Leen Wehbeh, Sama Alreddawi, Roberto Salvatori
Expert Review of Endocrinology & Metabolism.2019; 14(3): 167. CrossRef - Xanthomatous Hypophysitis Is Associated with Ruptured Rathke’s Cleft Cyst
Kai Duan, Sylvia L. Asa, Daniel Winer, Zadeh Gelareh, Fred Gentili, Ozgur Mete
Endocrine Pathology.2017; 28(1): 83. CrossRef - Xanthomatous Hypophysitis Presenting with Diabetes Insipidus Completely Cured Through Transsphenoidal Surgery: Case Report and Literature Review
Wei Lin, Lu Gao, Xiaopeng Guo, Wenze Wang, Bing Xing
World Neurosurgery.2017; 104: 1051.e7. CrossRef - Review of xanthomatous lesions of the sella
B.K. Kleinschmidt‐DeMasters, Kevin O. Lillehei, Todd C. Hankinson
Brain Pathology.2017; 27(3): 377. CrossRef - Xanthomatous hypophysitis
Bishoy Hanna, Yan M. Li, Timothy Beutler, Parul Goyal, Walter A. Hall
Journal of Clinical Neuroscience.2015; 22(7): 1091. CrossRef - Clinical Characteristics, Management, and Outcome of 22 Cases of Primary Hypophysitis
Sun Mi Park, Ji Cheol Bae, Ji Young Joung, Yoon Young Cho, Tae Hun Kim, Sang-Man Jin, Sunghwan Suh, Kyu Yeon Hur, Kwang-Won Kim
Endocrinology and Metabolism.2014; 29(4): 470. CrossRef - Brief Review of Articles in 'Endocrinology and Metabolism' in 2013
Won-Young Lee
Endocrinology and Metabolism.2014; 29(3): 251. CrossRef
- Xanthomatous hypophysitis causing hypogonadotropic hypogonadism resulting in delayed presentation of slipped capital femoral epiphysis
- A Case of Fetal Alcohol Syndrome with Secondary Amenorrhea.
- Yoon Young Cho, Hyo Jin Oh, Seok Jae Han, Sang Hun Sung, Gyu Hwan Bae, Ho Sang Shon, Hyun Dae Yoon
- J Korean Endocr Soc. 2005;20(5):524-530. Published online October 1, 2005
- DOI: https://doi.org/10.3803/jkes.2005.20.5.524
- 1,727 View
- 22 Download
- 1 Crossref
-
Abstract
PDF
- Alcohol ingestion during pregnancy can be damaging to embryonic and fetal development. A specific pattern of malformation, identified as Fetal alcohol syndrome, has been documented in 1~2 of every 1,000 live infant births Fetal alcohol syndrome is characterized by growth deficiency, facial abnormalities, cardiac defects, minor joint and limb abnormalities, as well as central nervous system dysfunction, including microcephaly, mental retardation and abnormal neurobehavioral development. However, there are few reports of fetal alcohol syndrome associated with hormonal abnormality or amenorrhea. Recently, a case of secondary amenorrhea, which developed in a 19-year-old woman with fetal alcohol syndrome, was experienced at our institute, but the exact cause of the amenorrhea was difficulty to find. Herein, this case is reported, with a review of the literature.
-
Citations
Citations to this article as recorded by- Alcohol Use during Pregnancy and Related Risk Factors in Korea
So Hee Lee, Seung Ju Shin, Seong-Du Won, Eun-Ju Kim, Dong-Yul Oh
Psychiatry Investigation.2010; 7(2): 86. CrossRef
- Alcohol Use during Pregnancy and Related Risk Factors in Korea
- A Case of Primary Aldosteronism with Aortic Dissection.
- Jung Hyun Seo, Ji Young Kim, Young Sup Kim, Wan Suk Kim, Jin Hyang Shin, Dong Jik Ahn, Yoon Young Cho, Sung Hwan Park, Jae Bok Park, Hyun Dae Yoon, Ji Hyun Lee, Ho Sang Shon
- J Korean Endocr Soc. 2004;19(4):452-457. Published online August 1, 2004
- 1,120 View
- 20 Download
-
Abstract
PDF
- Hypertension and atherosclerosis are the most important factors contributing to the development of aortic dissection. Primary aldosteronism is a rare cause of hypertension. The concurrence of aortic dissection is very rare in primary aldosteronism. However, when aortic dissection is found as a life-threatening complication of primary aldosteronism, then the diagnosis of primary aldosteronism is important because the therapeutic intervention can be curative. Only 3 cases of primary aldosteronism with aortic dissection have been reported in the literature. We report here on a case of primary aldosteronism with aortic dissection, which was treated by laparoscopic adrenalectomy. We lowered the blood pressure with antihypertensive drugs and potassium replacement was done to treat the aortic dissection. After stabilization of aortic dissection, we removed his left adrenal mass by laparoscopic adrenalectomy. Postoperatively, the patient's blood pressure has been within normal limits and the serum potassium increased to a normal level without supplementation. The aortic dissection has remained in a stable state
 First
First Prev
Prev


